Version 1
: Received: 7 July 2022 / Approved: 8 July 2022 / Online: 8 July 2022 (05:01:43 CEST)
Version 2
: Received: 21 July 2022 / Approved: 22 July 2022 / Online: 22 July 2022 (03:08:59 CEST)
Boudet, S.; Houzé de l’Aulnoit, A.; Peyrodie, L.; Demailly, R.; Houzé de l’Aulnoit, D. Use of Deep Learning to Detect the Maternal Heart Rate and False Signals on Fetal Heart Rate Recordings. Biosensors 2022, 12, 691, doi:10.3390/bios12090691.
Boudet, S.; Houzé de l’Aulnoit, A.; Peyrodie, L.; Demailly, R.; Houzé de l’Aulnoit, D. Use of Deep Learning to Detect the Maternal Heart Rate and False Signals on Fetal Heart Rate Recordings. Biosensors 2022, 12, 691, doi:10.3390/bios12090691.
Boudet, S.; Houzé de l’Aulnoit, A.; Peyrodie, L.; Demailly, R.; Houzé de l’Aulnoit, D. Use of Deep Learning to Detect the Maternal Heart Rate and False Signals on Fetal Heart Rate Recordings. Biosensors 2022, 12, 691, doi:10.3390/bios12090691.
Boudet, S.; Houzé de l’Aulnoit, A.; Peyrodie, L.; Demailly, R.; Houzé de l’Aulnoit, D. Use of Deep Learning to Detect the Maternal Heart Rate and False Signals on Fetal Heart Rate Recordings. Biosensors 2022, 12, 691, doi:10.3390/bios12090691.
Abstract
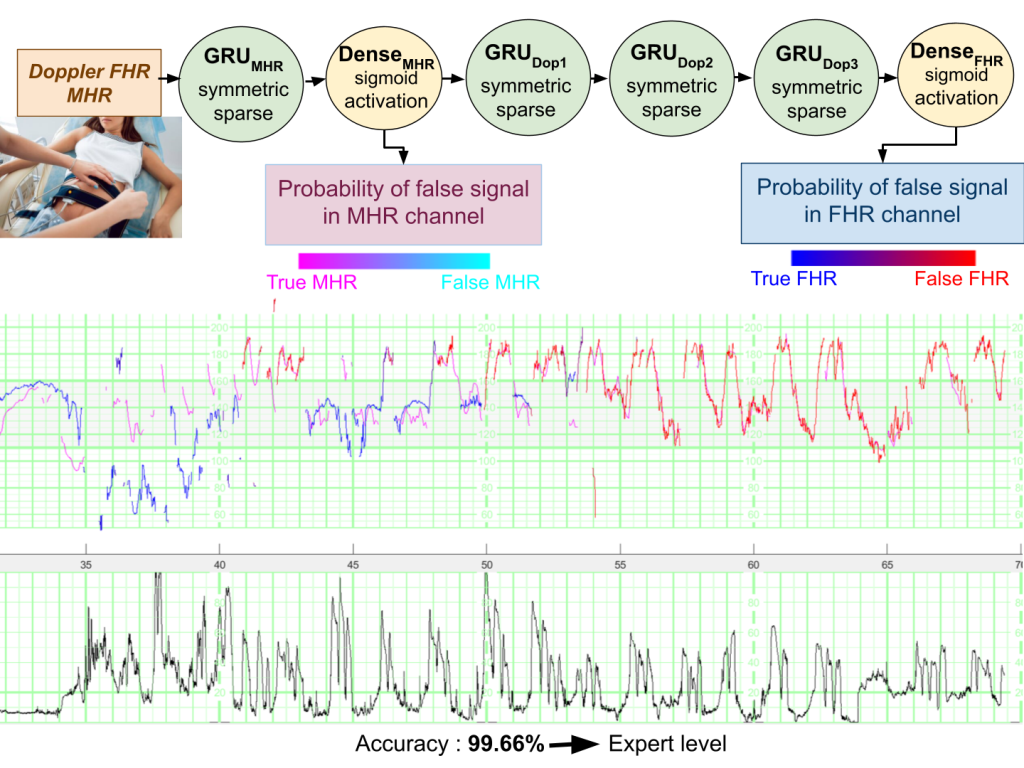
We have developed deep learning models for automatic identification of the maternal heartrate (MHR) and, more generally, false signals (FSs) on fetal heart rate (FHR) recordings. The modelscan be used to preprocess FHR data prior to automated analysis or as a clinical alert system to assistthe practitioner. Three models were developed and used to detect (i) FSs on the MHR channel (theFSMHR model), (ii) the MHR and FSs on the Doppler FHR sensor (the FSDop model), and (iii) FSson the scalp ECG channel (the FSScalp model). The FSDop model was the most useful because FSsare far more frequent on the Doppler FHR channel. All three models were based on a multilayer,symmetric, GRU and were trained on data recorded during the first and second stages of delivery.The FSMHR and FSDop models were also trained on antepartum recordings. The training datasetcontained 1030 expert-annotated periods (mean duration: 36 min) from 635 recordings. In an initialevaluation of routine clinical practice, 30 fully annotated recordings for each sensor type (meanduration: 5 h for MHR and Doppler sensors, and 3 h for the scalp ECG sensor) were analyzed. Thesensitivity, positive predictive value (PPV) and accuracy were respectively 62.20%, 87.1% and 99.90%for the FSMHR model, 93.1%, 95.6% and 99.68% for the FSDop model, and 44.6%, 87.2% and 99.93%for the FSScalp model. We built a second test dataset with a more solid ground truth by selecting 45periods (lasting 20 min, on average) on which the Doppler FHR and scalp ECG signals were recordedsimultaneously. Using scalp ECG data, the experts estimated the true FHR value more reliably andthus annotated the Doppler FHR channel more precisely. The models achieved a sensitivity of 53.3%,a PPV of 62.4%, and an accuracy of 97.29%. In comparison, two experts (blinded to the scalp ECGdata) respectively achieved a sensitivity of 15.7%, a PPV of 74.3%, and an accuracy of 96.91% anda sensitivity of 60.7%, a PPV of 83.5% and an accuracy of 98.24%. Hence, the models performed atexpert level (better than one expert and worse than the other), although a well-trained expert withgood knowledge of FSs could probably do better in some cases. The models and datasets have beenincluded in the Fetal Heart Rate Morphological Analysis open-source MATLAB toolbox and can beused freely for research purposes.
Computer Science and Mathematics, Mathematical and Computational Biology
Copyright:
This is an open access article distributed under the Creative Commons Attribution License which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

 ,
,
,
,
,
,
,
,





Commenter: Samuel Boudet
Commenter's Conflict of Interests: Author